
The Paradox of Risk: A Systemic Evaluation of AANHPI Mental Wellbeing, Stress Resiliency, and Vulnerability in San Diego County with Miramar College
Authors: Wilches, N.
Published: March, 2026
Executive Summary
This applied research report, offers a comprehensive examination of the psychological landscape characterizing the Asian American, Native Hawaiian, and Pacific Islander (AANHPI) population in San Diego County. Commissioned to contextualize the findings of recent evaluations at San Diego Miramar College and to support the strategic objectives of the San Diego Foundation, this document investigates a critical public health anomaly: the "Paradox of Risk."
Our central thesis posits that the AANHPI population exhibits a distinctive divergence between functional markers of success and internal markers of distress. While often perceived as the "model minority", characterized by high academic achievement, strong family cohesion, and self-reported wellness, this demographic is simultaneously experiencing a silent epidemic of high internalization, suicidal ideation, and a pervasive sense of external control.
Drawing upon the MindArch Health "5-Elements of Systemic Wellbeing" framework, recent social determinants of health data, and survey results from the Miramar College AANHPI Student Achievement Program, we identify the complex profile of this population (considering culture, economic, and community differences) through more precise data analysis to support differentiation. This report analyzes the 56% spike in youth suicide rates, the disproportionate burden on Southeast Asian students, and the specific protective factors that must be bolstered to avert crisis. It serves as a blueprint for moving from reactive clinical models to proactive, culturally responsive systemic wellbeing.
1. The Sociodemographic Landscape of San Diego's AANHPI Community
To understand the mental health of a population, one must first understand the structural reality in which they live. The AANHPI community in San Diego County is not a monolith; it is a complex, stratified mosaic comprising over 530,681 individuals, representing 16.2% of the region’s total population. This demographic weight makes San Diego the seventh-largest AANHPI hub in the nation, yet the aggregate numbers often obscure the critical nuances necessary for effective population health intervention within the community college context.
1.1 The Myth of Homogeneity
The label "AANHPI" aggregates groups with vastly different histories, economic realities, and health outcomes. In San Diego, the Filipino community stands as the largest single-race subgroup, accounting for roughly 4.4% of the county population, followed by Chinese, Vietnamese, and Indian communities. However, a significant and often overlooked demographic is the "Multiracial AANHPI" population, which is the second-largest category. This group, with a median age of just 22, represents the future of this demographic but faces unique identity challenges that are distinct from the first-generation immigrant experience.

Image 1 Source: MindArch Health
The visual representation above underscores the diversity that aggregate statistics often hide. While Filipino and Multiracial groups dominate, smaller populations such as the Cambodian, Laotian, and Hmong communities face specific, often acute, vulnerabilities related to historical trauma and refugee status. In San Diego, the discrepancy in economic power is stark: Asian Indian households command a median income nearly triple that of Cambodian households. This economic bifurcation means that a "one-size-fits-all" mental health strategy will inevitably fail; the stressors impacting a wealthy, tech-employed immigrant in Carmel Valley are fundamentally different from those impacting a housing-insecure Pacific Islander family in City Heights.
1.2 The Miramar College Microcosm
Our recent evaluation focused on the student population at San Diego Miramar College, a key community institution in the region’s educational ecosystem. The demographic profile of the survey respondents offers a crucial insight into the specific subset of the AANHPI population engaging with community college resources.
Analysis of the respondent race distribution reveals a significant skew: Southeast Asians comprise 43.6% of the survey respondents, followed by East Asians at 12.1% and Asians (unspecified) at 8.7%. This overrepresentation of Southeast Asian students, primarily Vietnamese and Filipino, is significant. These groups are historically more likely to be first-generation college students and to come from families with histories of refugee status or labor migration. As a result, perhaps more likely to attend community college than a four year institution.
Furthermore, the "Childhood Income Distribution" data indicates that a substantial portion of this population comes from "Average" or "Below Average" economic backgrounds, with very few identifying as "Far Above Average." This aligns with the "Work Status Distribution", where roughly 35% of respondents are employed part-time while studying, and nearly 30% are unemployed and not caring for others, likely focusing entirely on their studies. This profile represents an economically striving, working-class, and heavily Southeast Asian population and sets the stage for the specific pressured dynamics of the mental health paradox we observe.
2. The Mental Health Paradox: Perception vs. Reality
The core finding of our research is the disturbing disconnect between how AANHPI youth appear to function and their actual psychological state. This "Paradox of Risk" is characterized by high levels of performance and self-reported wellness masking severe, often lethal, distress.
2.1 The Divergence in Suicide Trends
Suicide statistics serve as the grim "canary in the coal mine" for systemic mental health failures. While the overall suicide rate in San Diego County has been trending downward, with a 12% decrease in deaths from 2019 to 2023, the data for youth tells a radically different story. Between 2022 and 2023, the suicide rate for youth aged 10 to 24 spiked by 56%.
This divergence is not random. It is driven disproportionately by vulnerable subgroups, with AANHPI youth and young adults at the epicenter. Suicide is now the leading cause of death for Asian American youth aged 15-24 and the second leading cause for Native Hawaiian and Pacific Islander youth. The fact that AANHPI youth are more likely to die by their own hand than by any other cause suggests the critical need to strengthen current support systems.
2.2 The "Model Minority" Mask
The paradox is further complicated by the fact that this distress is hidden. In the 2024 TAAF Youth Mental Health Study, nearly 70% of AANHPI participants described their mental health as "good" or "excellent." Yet, in the same cohort, nearly half (48%) scored above the clinical threshold for moderate depression on the PHQ-9 screening tool.
This gap between perception (70% healthy) and clinical reality (48% depressed) is the "Model Minority" mask in action. It suggests that AANHPI youth have normalized high levels of stress and dysphoria, viewing them not as symptoms of illness but as the necessary cost of achievement. They may not report being "unhealthy" because they are still functioning, attending classes, passing exams, and fulfilling family responsibilities. It is only when the internal pressure becomes unbearable that the system collapses, often without warning.

Image 2 Source: MindArch Health
The chart above illustrates this dissonance. The high rate of suicide planning and attempts (30% lifetime prevalence) coexists with a majority self-assessment of "Good/Excellent" health. This indicates a dangerously high threshold for pain and a lack of mental health literacy regarding what constitutes "wellness."
3. Theoretical Frameworks: Mechanisms of Distress
To effectively intervene, we must move beyond describing what is happening to understanding why it is happening. MindArch Health employs a multi-dimensional theoretical framework that integrates cultural psychology with systems theory. Two key constructs are essential for understanding the San Diego AANHPI population: Locus of Control and Internalization.
3.1 The "Poor External Locus of Control" Paradox
Locus of Control (LOC) refers to an individual’s belief system regarding the causes of their life events. In Western psychology, an "Internal Locus of Control" (the belief that one is the master of their own fate) is typically associated with resilience. An "External Locus of Control" (the belief that powerful others, fate, or chance determine outcomes) is often linked to helplessness and depression.
However, for the AANHPI population, the dynamic is more complex. Internally, many AANHPI students possess high internal Self-Efficacy - “I understand to make good decisions that will achieve positive outcomes” (internal trait) but poor external Self-Efficacy - “things happen to me that make or break my success” and “I do things because I have to not because I want to”. In this sense, people may feel their life's trajectory, such as their career choice, their marriage prospects, their role in the family, are controlled by external forces (parents, cultural expectations, economic necessity).
This creates a "Maladaptive Hybrid":
High Responsibility (Internal): e.g. "I hold principles about what I believe is important"
Low Autonomy (External): "I cannot plan, organize, and complete the steps toward my own goals."
This suggests that the student could be working incredibly hard to achieve a goal they did not choose. If they succeed, the credit is externalized to the family values ("I did it for them"). If they fail, the blame is internalized ("I am not good enough"). This specific combination could be highly problematic. It strips the individual of the joy of achievement while burdening them with the full weight of failure without the support to cope effectively.
The 5-Elements of Systemic Wellbeing Framework defines internal factors in the “Decided” Element related to self-efficacy as perceptions that one has insight, control, values, mindset, perception and reasoning.

Image 3 Source: MindArch Health
The 5-Elements of Systemic Wellbeing Framework defines external factors in the “Decided” Element related to self-efficacy as having positive intention, attitude, habits, process, effort, influence over their circumstances.

Image 4 Source: MindArch Health
3.2 Internalization and the "Pressure Cooker"
Internalization is the psychological process of turning negative emotions inward rather than expressing them outwardly. While externalizing behaviors (refusal, poor attendance, acting out) are often flagged by educators and parents as "problematic," internalizing behaviors (quiet withdrawal, somatic pain, self-criticism) can be rewarded in some AANHPI cultures as signs of "maturity" or "discipline."
High internalization is the mechanism that hides the suicide risk. The student who is planning suicide is often the same student who is quiet, polite, and earning good grades. They are containing their distress to avoid burdening the collective unit (the family). This containment creates a "pressure cooker" effect. Without an outlet for emotional regulation, what MindArch terms the “Regulated” element, the pressure builds until the containment vessel shatters.
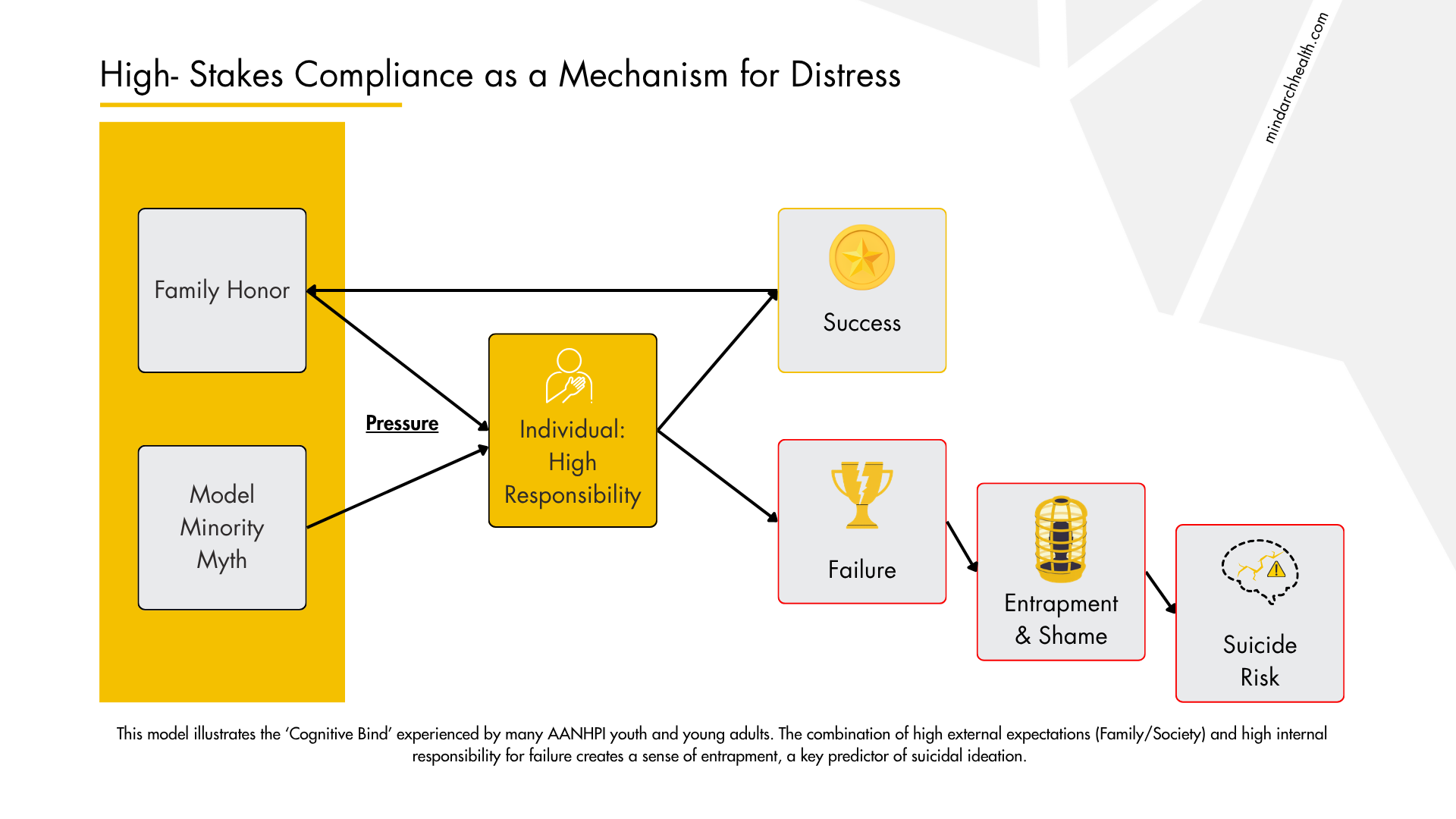
Image 4 Source: MindArch Health
3.3 The 5-Elements of Systemic Wellbeing Framework
MindArch Health moves beyond the deficit (pathogenic) model to assessing the presence of health (salutogenic). Our framework defines five key resiliency factors:
Secure: The foundational sense of safety, stability, and belonging.
Regulated: The ability to manage emotional states and maintain healthy biological routines.
Valued: The perception of being significant, worthy, and respected.
Decided: The sense of self-efficacy, agency, and the ability to influence one's environment.
Related: The quality of interpersonal connections and social support.
In the context of the AANHPI population, we hypothesize a specific imbalance: High “internal” Decided (efficacy) but Lower Secure (anxiety/safety) and Conditional Valued (worth dependent on success).
4. MindArch Health Evaluation: Findings from the Miramar College Cohort
MindArch Health conducted a comprehensive assessment of the AANHPI student population at Miramar College, utilizing both the Psychological Health Survey and the Protective Factors Survey. The results validate our theoretical model and provide granular data on the state of this community.
4.1 Respondent Profile: Southeast Asian Dominance
The survey captured a distinct slice of the AANHPI community. As noted in the analysis of Image 9, the largest group of respondents identified as Southeast Asian (43.6%), dwarfing East Asians (12.1%) and other groups. This is a critical finding for Miramar College. The mental health needs of Southeast Asian students, many of whom are Vietnamese, Filipino, Cambodian, or Laotian, are often linked to intergenerational trauma from war and displacement, which differs significantly from the "immigrant striving" narrative often applied to East Asian groups.
The Gender Distribution (Images 4 & 5) was relatively balanced but showed a higher participation rate among women (55.7% female at birth) compared to men (43.6%). Notably, 1.3% identified as Transgender and 0.7% as Non-binary. While small percentages, these represent real students who, according to national data, are at the highest risk for suicidality within the AANHPI umbrella.
4.2 The 5-Elements Profile: High Function, Hidden Risk
The aggregated scores for the population present a picture of resilience mixed with vulnerability.
Decided (Score: 76 Psychological / 70 Protective): A divergence here shows high internal understanding of their efficacy but lower external control over their circumstances offering the biggest opportunity for strengthening protective factors leading to a goal in this area.
Secure (Score: 70 Psychological / 68 Protective): This was among the lower scores, particularly on the Protective Factors side. A score of 68 in "Secure" indicates that the environment is not providing adequate safety. This aligns with the high rates of discrimination and lack of feeling protected or a perceived lack of equity. The students' lack of psychological safety can contribute to a feeling of lack of control over their decisions.
Regulated (Score: 68 Psychological / 69 Protective): The lowest score on the psychological survey. This confirms the "Internalization" hypothesis. Students are struggling to regulate their emotions, likely suppressing them until they become unmanageable.
Valued (Score: 69 Psychological / 70 Protective): A moderate score, suggesting that while students feel some sense of worth, it may be precarious due to suicide risk levels.
Related (Score: 74 Psychological / 69 Protective): A divergence here is also notable. Psychologically, students feel "Related" (perhaps due to strong family or community bonds), but the Protective Factor score is lower (69). This suggests that while the bonds exist, they may not be protective in the context of mental health i.e., you may not be able to express your thoughts and feelings to others.
4.3 The Predictive Goal: "Increase Decision by Improving Beneficial Habits"
The MindArch algorithms generated a specific predictive goal for this population: Increase Decision By improving Beneficial Habits.
At first glance, this seems contradictory. We suggested that this population scored higher in the "Decided" element. The nuance lies in the definition of "Decision" within the Protective Factors framework. Here, "Decision" relates to agency, the ability to make choices that align with one's own wellbeing. The "Habits" component refers to the daily routines (sleep, exercise, study) that support that agency.
The system is detecting that while students feel internally decided, they do not feel a sense of agency over their daily habits and routines that could meet their internal wellbeing needs and goals. The recommendation to strengthen healthy habits that give agency to students, allowing them to feel more secure and regulated.
5. Risk Factors and Systemic Vulnerabilities
The evaluation identified specific systemic vulnerabilities that exacerbate the risk for this population. These align with the "9 Vulnerability Categories" tracked by MindArch Health.
5.1 Economic Disadvantage and Housing Insecurity
While the "Model Minority" myth assumes affluence, the Miramar data contradicts this. The "Childhood Income Distribution" (Image 3) shows a bell curve skewed toward the lower end, with significant portions of the population in "Below Average" or "Far Below Average" categories. This is relatively common for students attending community college.
Furthermore, county-level data indicates that Native Hawaiian and Pacific Islander (NHPI) populations face severe housing insecurity, with only 17% homeownership compared to 74% for other groups. For a student, housing insecurity attacks the Secure element directly. It is extremely difficult to focus on "Self-Actualization" when "Physiological Safety" is threatened.
5.2 Discrimination and Bullying
The San Diego context includes a reported rise in anti-Asian hate crimes. For the AANHPI population, discrimination is a pervasive background radiation. 93% of AANHPI youth reported race-based discrimination in the past year. This creates a state of chronic hyper-vigilance. The "Secure" score of 68 is likely a direct reflection of this. When a student walks onto campus, they are scanning for threats. This cognitive load depletes the energy available for emotional regulation and forces decision making that may contradict personal motivations.
6. The "Decided" Paradox: Agency Without Power
The central paradox: Why does a population that scores high on "Decided" (Self-Efficacy) have such "Poor External Locus of Control"?
Considering the high rates of historical trauma and refugee status, housing and other economic challenges, high rates of discrimination, and poor emotional regulation and psychological safety, it becomes more clear why students’ feel internally “decided” but unable to actualize those decisions. While attending classes, many of these students are also working part time and all of them are commuting. They are decided. But the locus of that decision often resides outside of them.
This creates a Fragile Agency. If they struggle academically, they are not just failing a class; they are failing their ancestors, and the sacrifices made to help them attend college. This transforms a minor academic setback into a catastrophic identity crisis. The "poor external locus of control" means they feel they cannot change the script. They cannot say, "Actually, I want to be an artist," because the external control (economic necessity/family honor) is perceived as absolute.
When the pressure to fulfill this external script exceeds the student's internal capacity to cope (Regulation), and they feel they cannot change the script (External Locus), suicide can be perceived as the only available act of autonomy. This is the terrifying conclusion of the paradox.
7. Strategic Interventions: The Miramar Model
The interventions piloted at San Diego Miramar College represent a paradigm shift from the traditional "clinical-reactive" model to a "community-proactive" model. Recognizing that AANHPI students often avoid formal mental health services due to stigma and the "Model Minority" pressure, the Miramar Model employs a "de-colonizing" approach. This strategy moves away from a one-size-fits-all methodology, which often centers Western clinical norms, toward a strength-based model that honors individual agency and lived experience.
7.1 The "Soft Entry" Approach: De-stigmatizing Care
The core of this strategy is the implementation of bi-weekly psychosocial workshops. Unlike clinical group therapy, which implies pathology, these workshops are framed as community-building and skill-sharing spaces. They are tailored specifically to the Miramar experience, developed based on direct student feedback to ensure relevance.
Peer-Led Trust: The program is coordinated by an alumnus of the system (SDSU/Masters level), rather than an external clinician. This shared identity reduces the power differential often found in therapy, establishing immediate trust.
Community over Isolation: By strengthening the "community aspect" of support rather than solely individual counseling, these workshops combat the isolation inherent in the "Decided" element paradox discussed in Section 6. The success of this model is evident in the sustained attendance of 20+ students per session.
7.2 Intersectionality and Visibility
To address the "hidden" nature of AANHPI distress, the Miramar Model increases visibility through "tabling" at psychosocial and market events and within the resource center. This normalizes mental health presence in everyday student life. Furthermore, the model explicitly addresses intersectional identities, specifically the LGBTQ+ AANHPI population, through cross-over programming with the new Pride Center. This acknowledges that students exist at the intersection of multiple vulnerabilities and requires a unified support system.
7.3 Systemic Integration: Technology and Access
Recognizing that economic disadvantage and time constraints (work/commute) are major stressors, the intervention integrates support directly into the student's existing digital and financial ecosystem:
Preventive Technology: The provision of free Headspace subscriptions allows for private, self-paced emotional regulation training, directly addressing the low "Regulated" scores identified in the survey.
Institutional Alignment: Mental health is not treated as a silo; it is integrated with Counseling and Financial Aid services to address the root causes of anxiety (e.g., housing/tuition stress).
Digital Accessibility: A campus resource hub is embedded in every student's Learning Management System (LMS) account, ensuring that help is available where students spend the majority of their academic time.
8. Recommendations: From Awareness to Systemic Action
The data is clear: the AANHPI population in San Diego is resilient but structurally vulnerable. To address the paradox of high suicide rates amidst high achievement, we must shift our focus from "treating symptoms" to "building capacity" in the Secure and Regulated domains.
8.1 For Educational Institutions (Miramar College)
Integrate "Beneficial Habits" into Curriculum: The predictive goal was to "Increase Decision by improving Beneficial Habits." Colleges should integrate "Life Design" or "Wellness" modules into the mandatory freshman orientation, teaching regulation skills (sleep, stress management) as academic skills essential for success, rather than as "soft" skills.
Disaggregate Data Continuously: Continue to track Southeast Asian students separately. Their economic and historical profile differs from East Asian students, and their support needs may be more rooted in financial aid and first-generation navigation.
Empower the "Internal Locus": Career counseling should focus on "Value Alignment." Helping students connect their career choices to their own values (rather than just family duty) can help shift the Locus of Control from External to Internal, reducing the sense of entrapment.
8.2 For The System (District & Supporting Foundations)
Invest in the "Missing Middle": The Multiracial AANHPI population (median age 22) is growing rapidly. Funding should target programs that address the complexity of multiracial identity, as these youth often feel excluded from traditional single-ethnicity cultural organizations.
Scale the "Non-Clinical" Model: The success of the "Healing Circles" proves that clinical impact can happen in non-clinical settings. Expand funding for arts-based, food-based, and community-based mental health initiatives that lower the barrier to entry.
8.3 For MindArch Health & The Community
Validate the Paradox: We must continue to publish data that challenges the "Model Minority" myth. The 56% spike in youth suicide is a call to action. We must educate parents and community leaders that "quiet" does not mean "okay," and that high grades can coexist with high risk.
Strengthen the "Secure" Base: Community advocacy against anti-Asian hate and gun violence is not just political; it is a mental health intervention. Reducing the baseline anxiety of the population will directly improve the "Secure" score, freeing up cognitive resources for resilience.
Conclusion
The AANHPI community in San Diego is a testament to the power of resilience. They are "Decided," hardworking, and deeply "Related" to their families. But they are also carrying a heavy, invisible load. The "Paradox of Risk", the coexistence of success and suicide, is sustained by silence and the pressure to conform to external expectations.
By applying the MindArch 5-Elements framework, we can see the cracks in the foundation: the lack of "Security" and "Regulation" that threatens to topple the structure. The interventions at Miramar College prove that we can fill these cracks. By creating spaces where students are Valued for who they are, not just what they achieve, and by providing the tools to Regulate the immense pressure they feel, we can shift the Locus of Control back to the individual. We can turn "Agency without Power" into true, systemic wellbeing.
____________________________________________________________________________________
Data Sources: San Diego Foundation, San Diego County HHSA, TAAF, CDC, MindArch Health Internal Data, Miramar College AANHPI Student Achievement Program Reports.
Works cited
Beyond the Surface: Youth Mental Health Study 2024 - The Asian American Foundation, accessed January 23, 2026, https://www.taaf.org/youthmentalhealth
Breaking the Silence: An Epidemiological Report on Asian American and Pacific Islander Youth Mental Health and Suicide (1999-2021) - PubMed, accessed January 23, 2026, https://pubmed.ncbi.nlm.nih.gov/38525866/